


140 |
F. Collettini and B. Hamm |
|
|
which are histologically similar to carcinomas of the uterine corpus. They are of an intermediate to slightly high signal intensity on MRI and arise in the endocervix, from where they infiltrate the cervical stroma. In this type of tumor, it may be difficult to determine whether the origin is in the cervix or in the uterine corpus. In general, the part of the uterus from which the tumor arises shows deeper infiltration and more marked enlargement to the respective other part (cervix or corpus). The rare subtype of adenosquamous cervical carcinoma resembles squamous cell carcinoma with regard to its growth pattern and morphologic appearance on MR images.
Neuroendocrine cervical carcinoma is the second most frequent of the rare histologies. With its heterogeneous appearance and high signal intensity on T2-weighted images, neuroendocrine cervical carcinoma resembles squamous cell carcinoma at MRI (Lopes Dias et al. 2015).
2.3.3\ Tumor Size
Cervical cancer is revealed by MRI when tumors are large enough to be macroscopically visible, which is the case when the tumor has a diameter of 1–2 cm or a volume of 2–4 cm (Cancer Research UK 2016) (FIGO stage IB). Tumor size is the most important prognostic factor besides lymphatic metastasis. T2-weighted MRI in at least two planes is the method of first choice for determining tumor size (Hawighorst et al. 1997), since cervical cancer is best distinguished from surrounding tissue in these sequences. While gynecologic examination tends to underestimate tumor size with reported accuracy rates as low as 60%, MR imaging is very accurate in evaluating tumor size with 93% of cases within 5 mm of the histologic size (Hricak et al. 1988; Mitchell et al. 2006; Shiraiwa et al. 1999; Lopes Dias et al. 2015; Nicolet et al. 2000; Okamoto et al. 2003; Sahdev et al. 2007). Exact assessment of tumor size is crucial not only in patients with early-stage cervical cancer scheduled for fertility-sparing surgery, but also for patients with stage IIA cervical cancer or less, since patients with tumors larger than 4 cm are considered nonsurgical candidates. Preliminary comparative studies have shown that tumor delineation and determination of size
can be further enhanced by contrast medium administration. Preliminary comparative studies have shown that contrast-enhanced T1-weighted imaging may by superior to T2-weighted imaging in terms of cervical cancer localization and tumor margin detection, especially in patients with small tumors (Akita et al. 2011).
Tumor size is usually determined by measuring the longest diameter and its perpendicular. Two-dimensional measurement is based on the WHO guidelines for evaluating the response of solid tumors to chemotherapy or radiotherapy. Since a precise description of the spatial extent of a tumor is crucial prior to surgery, the tumor should also be measured in the third dimension. In patients where it is important to evaluate the response to radiochemotherapy, tumor size should be measured according to the revised RECIST1 (response evaluation criteria in solid tumors) guideline which uses one-dimensional measurements (Eisenhauer et al. 2009) (Fig. 13). These guidelines have superseded the twodimensional WHO measurement as the standard.
Techniques of tumor volumetry can additionally be applied. These techniques relied on formula such as height × width × length × π/6 to calculate approximate tumor volume or determined the volume by integration of the individual slice volumes (Fig. 12).
2.3.4\ Local Staging
2.3.4.1 Stage IA
There is no role for MR imaging in patients with microinvasive cervical cancer (stage IA). Microinvasive cervical cancers do not alter the normal morphologic MR appearance of the cervix (Fig. 15). The normal endocervix is depicted on T2-weighted images with a hyperintense, continuous mucosal layer surrounded by hypointense cervical stroma, consisting of connective tissue and smooth muscle. Hence, imaging is optional in patients with tumors IB1 or lower. Colposcopy and conization are the
1RECIST is a set of rules defining the criteria for tumoral response, stability, or progression during treatment. The longest diameter of the non-nodal lesions is measured.
Cervical Cancer |
141 |
|
|
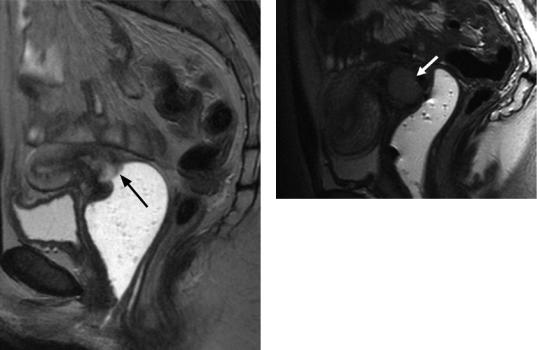
Fig.15 Stage IB. T2w TSE image in sagittal orientation. High-signal-intensity cervical cancer (arrow) primarily involving the anterior cervix and the portio. Gel filling of the vagina
methods of choice for evaluating these early forms of cervical carcinoma. The conization defect is depicted on MR images as a circumscribed lesion of the external os, quite often associated with an adjacent seroma or clot. In the further course, shrinkage of the portio can sometimes be seen.
2.3.4.2 Stage IB
Stage IB cervical carcinoma has a depth of more than 5 mm and a diameter of more than 7 mm or is visible clinically. The tumor is still confined to the cervix but is characterized by invasive local growth. This is the earliest stage that can be demonstrated by MRI (Mitchell et al. 2006). The average MRI detection rate is 95%. Stage IB1 (diameter <4 cm) and stage IB2 (diameter >4 cm) are distinguished based on their size. Stage IB2 cervical cancer has a poorer prognosis and should be treated with concomitant chemotherapy and radiation therapy. Transverse and sagittal T2-weighted images depict cervi-
Fig.16 Stage IB. T2w TSE image in sagittal orientation. High-signal-intensity cervical cancer (arrow) primarily involving the anterior cervix and the portio. Gel filling of the vagina
cal carcinoma as a highor intermediate-inten- sity lesion within the low-signal-intensity oval cervical stroma (Figs. 11, 16, 17, 18, and 19). Cervical cancer at this stage is fairly smoothly marginated and completely surrounded by low- signal-intensity cervical stroma. Occasional exophytic bulging of a stage IB tumor into the vagina or the parametrium may be mistaken for infiltration.
A large stage IB2 cervical carcinoma can obstruct the cervical canal and lead to hydrometra or hematometra. Hydroor serometra is suggested by a fluid collection in the uterine cavity showing hyperintensity in T2-weighted and low- signal-intensity in T1-weighted images, whereas a hematometra is characterized by high signal intensity in T2and T1-weighted images.
The rationale of using MR imaging at this stage of disease is to accurately assess tumor size, parametrial invasion, lower vaginal involvement, and lymph node metastases. Identification of this prognostic factors would preclude surgical treatment and is thus crucial for therapy planning (Freeman et al. 2013; Cheng et al. 2004; Kupets and Covens 2001).
2.3.4.3 Stage IIA
In stage IIA cervical cancer, infiltration involves up to two-thirds of the proximal vagina while sparing the lower third. On T2-weighted MR images, vaginal involvement is seen as a
142 |
F. Collettini and B. Hamm |
|
|
a |
b |
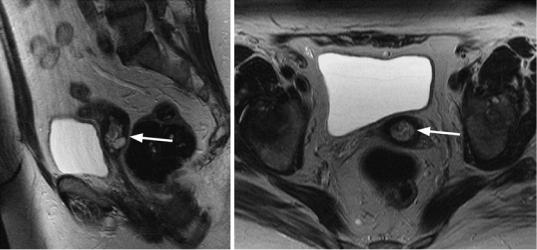
Fig. 17 Stage IB. (a, b) T2w TSE images in sagittal and transverse orientation. The cervical cancer is seen as a high-signal-intensity lesion within the cervix (arrows).
The cancer is surrounded by low-signal-intensity cervical stroma on both sagittal and transverse images. Accessory finding: Nabothian cysts
hyperintense segmental disruption or lesion in the otherwise low-signal-intensity vaginal wall. Infiltration of the anterior and posterior fornix and of the wall is best seen in sagittal orientation (Figs. 20, 21, 22, and 23). The radiologist interpreting the images must be aware that a large exophytic cervical cancer may lead to widening of the fornix and thus mimic vaginal infiltration. In such cases, opacification and distention of the vagina can be helpful. Similarly to stage IB, stage IIA is further subdivided into IIA1 (if the tumor is 4 cm or smaller in diameter) and IIA2 (for tumors greater than 4 cm in diameter). Stage IIA is further defined by the absence of parametrial invasion. Parametrial infiltration can be reliably excluded if the tumor is surrounded by a low- signal-intensity rim on transverse angulated T2-weighted images.
2.3.4.4 Stage IIB
Stage IIB cervical cancer is characterized by parametrial infiltration but without extension to the pelvic sidewall. Parametrial infiltration has important implications for the therapeutic approach. While gross parametrial invasion can be usually detected by experienced clinicians, early invasion usually remains undetected. Reported accuracy of clinical staging for detec-
tion of parametrial and pelvic side wall invasion amounts to only 29–53% (Hricak et al. 1988; Zand et al. 2007). MRI is the only noninvasive modality that allows adequate evaluation of parametrial infiltration with a reported sensitivity of 69%, specificity of 93%, and negative predictive values of 100% for depicting parametrial invasion (Zand et al. 2007). Sagittal and transverse T2-weighted images angulated perpendicular to the cervical canal are most suitable to evaluate parametrial infiltration. It is indicated by a disruption of the low-signal-intensity cervical stroma and tumoral extension into the parametria. Visualization of an uninterrupted rim of cervical stromal rim thicker than 3 mm (“hypointense rim sign”) reliably excludes parametrial infiltration with a specificity as high as 99% (Zand et al. 2007). The accuracy of MRI in the evaluation of parametrial invasion varies according to the tumor size, with 96% accuracy in small tumors and 70% in large tumors (Zand et al. 2007). Early microscopic parametrial infiltration must be suggested if high-signal-intensity tumor tissue shows irregular and unsharp margins and is disrupting the hypointense cervical stroma with no normal cervical stroma left that separates the tumor from the parametria. The most reliable MRI criterion of parametrial infiltration is the direct visualization

Cervical Cancer |
143 |
|
|
a b
c |
d |
Fig. 18 Stage IB. (a, b) T2w TSE images in sagittal and transverse orientation. High-signal-intensity lesion of the cervix (arrows) with preservation of low-signal intensity stroma around the tumor. (c, d) T1w TSE images in sagit-
tal and transverse orientation. No circumscribed cervical cancer is seen on the image obtained 1 min after Gd-DTPA administration. Accessory finding: uterine adenomyosis
of a tumor mass extending into the parametria (Figs. 24, 25, 26, and 27). Occasionally, the parametria may be invaded from below, through the paravaginal space. The anatomy of the true pelvis determines the further routes of spread of cervical cancer. Infiltration of the rectouterine or vesicouterine ligaments at their cervical attachments is seen on MR images as focal thickening. In rare cases, parametrial invasion can cause retraction with displacement of the cervix to the side of infiltration.
2.3.4.5 Stage IIIA
Stage IIIA tumor is established when there is involvement of the lower third of the vagina. As with stage IIA tumor, sagittal and oblique transverse T2-weighted sequences are most suitable to evaluate vaginal infiltration. Tumor infiltration is indicated by a hyperintense disruption and continuous or discontinuous thickening of the vaginal wall that extends to the lower third of the vagina. This stage is also associated with an increased risk of metastatic spread to the