

Lines and Tubes |
135 |
Fig. 7.1f Chondroblastoma on CT. Note the rib and spinal element destruction. Inclusion of two adjacent bones enters the infection differential
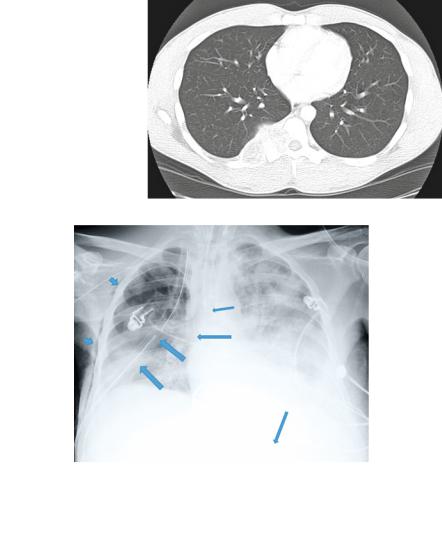
Fig. 7.2a This ICU patient has the ET tube a bit close to carina for my liking (within one cm; thinnest arrow near carina). The PICC line is seen entering from the right arm and entering the right brachycephalic, terminating (the tip) in the SVC (long arrow overlying mediastinum). A right chest tube is noted (widest arrows) with sideport (most superior arrow) and with tip in right apex. Subcutaneous emphysema is noted lateral to the ribs in the chest wall soft tissues (shortest arrows). NG tube is seen in stomach (long arrow over stomach)
Lines and Tubes
Several figures have included lines and tubes throughout this book. Please refer back to the abnormal parenchyma chapter, for example, placements of chest and ET (EndoTracheal Tubes), PICC, Port-a-Cath, IJ, and other central lines.
See Fig. 7.2a for many of the common lines found in typical ICUs.
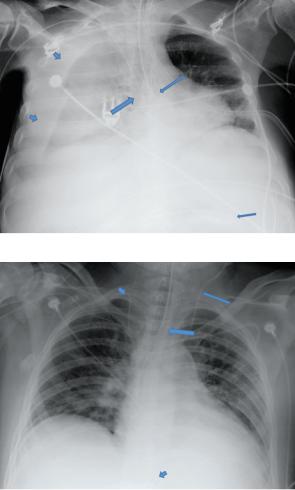
See Fig. 7.2b for a more worrisome picture of a failed right jugular line placement with a bleed into the right hemithorax. Also the ET tube was to distal, in the Right Mainstem Bronchus.
136 |
7 Abnormal Bones, Soft Tissue, and Other Findings |
Fig. 7.2b Example of a failed right jugular line placement with a bleed into the right hemithorax (wide short arrows). The ET tube was to the distal, in the right mainstem bronchus (long arrow). This causes further decreased aeration to the right lung (shut off from bypassing only aerating left lung). PICC line coming from right arm is okay in SVC (wide arrow). Also NG tube is okay coiled in stomach. Remainder of lines are ECG lines on patient
Fig. 7.2c Note the left IJ line (long arrow) enters brachiocephalic, then takes a turn to the left jugular (short arrow in left neck). The ET is a few centimeters above the carina (long wide arrow) and the NG tube is within the stomach (short arrow overlying stomach)
Figure 7.2c demonstrates how lines can go in many directions; to no fault of the faculty, staff, interns, residents, and fellows that place them. Malplacement is exactly why routine chest images are obtained.
One helpful tool I have used to help locate lines is by reversing the grayscale. A better recently development is called Tube and Line Visualization Software by Carestream Health (Rochester, NY). [2] that increases conspicuity of radiopaque devices (see Fig. 7.2d, e).
With portable DR (Direct Radiography) and instant viewing, ICU and other providers can instantly see their tube placements, now digitally enhanced to save trips to the PACS and/or radiology department. Also avoids waiting for a report or a call for a misplaced line or tube. Nonradiologists seem to favor the digitally enhanced
Lines and Tubes |
137 |
Fig. 7.2d,e This patient has a left-sided Swan catheter (too far lateral, should be a few centimeters from midline) in the right pulmonary artery, in addition to a right PICC line and ET tube (arrows). Note the lower image demonstrating increased conspicuity of the lines and tubes (special line and tube enhancement sofware). Also note the diffuse patchy airspace opacities that represented edema in this patient. The left hemidiaphragm is not well visualized, indicating effusion in this case
images. I call this process “digital solarization” as it is similar to what we used to do in the darkroom by turning the lights on halfway through development.
Another trick for quickly assessing for rib fractures is to invert the CXR; they stand out because our usual eye scanning is thrown off.
Lastly, do not forget to look at the abdomen as it is partially included in every CXR. See this last case where the patient also had a SBO (Small Bowel Obstruction).
Figure 7.3a and b highlights a few basic points. Look everywhere (the search pattern); think about everything (within reason, but region and pattern approach). This last case is a surgical emergency and must be recognized. When in doubt, get additional films and call someone more experienced than you.

138 |
7 Abnormal Bones, Soft Tissue, and Other Findings |
Fig. 7.3a Note the distended small bowel loops in the upper abdomen. This turned out to be an SBO
(see Fig. 7.3b)
Fig. 7.3b Note diffusely dilated small bowel loops. No large bowel loops are seen
References
1. Warnock A, Gibson M, Folio L. Chondroblastoma with secondary aneurysmal bone cyst. Mil Med Int J AMSUS. 2008;173(2):xiii–xiv.
2. Foos DH, Yankelevitz DF, Wang X, Berlin D, Zappetti D, Cham M, Sanders A, Parker KN, Henschke CI. Improved visualization of tubes and lines in portable intensive care unit radiographs: a study comparing a new approach to the standard approach. Clinical Imaging. 2011;35(5): 346–52.