


74 5 Surgical Extraction Techniques
Cementoenamel
junction
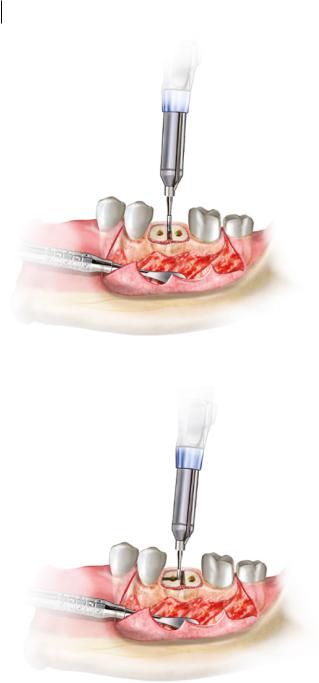
Figure 5.5 Buccal bone gutter to facilitate removal of a lower molar.
Planning where bone is to be removed depends on the desired outcome of the removal. In most cases, bone removal is undertaken to create a straight and open path of delivery for a tooth or tooth root (Figure 5.5). As such, the bone removed should be predominantly at the cementoenamel junction of the tooth, as wide as possible without damaging adjacent teeth, and only as apical as is required to bypass the thickest part of the tooth, all whilst enabling a point of access for instrumentation.
With the advent of immediate dental rehabilitation with endosseous implants, emphasis should be placed on the preservation of as much alveolar bone as possible. Adequate alveolar bone height and width can be maintained through techniques that, where possible, favour tooth sectioning over bone removal, in order to remove teeth.
Using an appropriate retractor, the soft tissues must be kept away from the site where bone is to be removed. A round or fissure bur attached to a surgical handpiece should be used to gently remove the bone around the desired area, starting from where the crown is visible. In nearly all cases, exposure of the entire crown to the cementoenamel junction is considered sufficient bone removal, although this can vary depending on the complexity of the case, and more or less may be required to obtain the desired outcome. Care must be taken not to drill into the tooth itself, as this can lead to loss of anatomy or difficulty in maintaining an application point, whilst at the same time creating a point of weakness that may lead to crown fracture. Irrigation should be used throughout bone removal to prevent thermal osteonecrosis, and surgical suction must be applied liberally to collect any irrigant and debris from the site.
5.5 Tooth Sectioning
Once a tooth’s crown is sufficiently exposed, and bone removal has provided sufficient exposure of the tooth roots and space for extraction, tooth sectioning should be performed, if required. Generally, tooth sectioning is utilised in three situations: crown removal, to create space to
https://t.me/DentalBooksWorld

5.6 alproSs ronfal ASPp 75
Bone gutter
Figure 5.6 Decoronation of a tooth.
facilitate root removal; sectioning between multirooted teeth; and sectioning axially along a sin- gle-rooted tooth.
Decoronation (separation of a crown from its roots) can assist in creating a path of exit when elevating the root in situations where the crown is impacted (Figure 5.6). Even when the crown is not impacted, removal can still be a useful technique to visualise the root anatomy of a multirooted tooth and provide additional access for further bone removal and sectioning. To decoronate a tooth, the cementoenamel junction should first be exposed from under any hard or soft tissue. A straight bur must be held perpendicularly to the tooth. The tooth can then be sectioned through the entire depth of the crown, taking care not to traverse through the crown into surrounding structures. The section should be completed using an elevator to remove the crown.
Sectioning between roots can be used for multirooted teeth, where each root may have a different vector of extraction (Figure 5.7). Sectioning between roots allows for extraction of each root individually, and reduces the risk of excessive force on alveolar bone. It is easiest to perform (although this is not absolutely necessary) after decoronation of a tooth, as pulp and root anatomy is easier to identify, and access to the interradicular areas of the root system is far simpler. An understanding of the root anatomy and recognition of the variations in the preoperative assessment is essential when undertaking root sectioning. If roots are not sectioned according to tooth anatomy, undesirable fractures of root tips can occur, leading to a much more complex and lengthy procedure.
Sectioning within a single root is usually reserved for canine teeth, where a wide single-rooted tooth with a large periodontal ligament area is resistant to removal and the surrounding alveolar bone is thick and unforgiving (Figure 5.8). In order to preserve alveolar bone, the tooth may be sectioned axially through the pulp chamber. This allows each half of the root to be luxated into the resultant space and elevated separately. Sectioning in such a fashion is an advanced skill, but when appropriately utilised, it significantly improves the prognosis of the area for future prosthetic rehabilitation.
5.6 Cleanup and Closure
Once a tooth has been extracted, the socket should be examined for any tooth remnants, debris, or iatrogenic damage to the periodontal bone or soft tissues. This involves gently irrigating the socket
https://t.me/DentalBooksWorld
76 5 Surgical Extraction Techniques
Figure 5.7 Sectioning between roots.
Figure 5.8 Sectioning within a single root.
with 5–10 ml of normal saline; if any periodontal plaque or calculus is noted on the adjacent teeth, these areas should be gently curetted to reduce the risk of postoperative infection.
The socket and surrounding areas should be checked for any frank bleeding that may need to be addressed. A transient ooze is expected following extraction, but prolonged bleeding lasting more than five minutes requires active management. If there is bleeding from alveolar bone after an
https://t.me/DentalBooksWorld
5.6 Cleanup and Closurp 77
uncomplicated extraction, the precise source must first be discovered. A resorbable gelatinor cellulose-based dressing can then be packed against the area.
The final step in surgical extraction is closure of the socket. Using interrupted sutures, any soft tissue flaps must be repositioned to their original locations, with a particular emphasis on restoring the periodontal contour of the alveolus. The socket itself can be left slightly open to facilitate surgical drainage from the site, which can reduce postoperative pain and swelling.
https://t.me/DentalBooksWorld
https://t.me/DentalBooksWorld

79
6
Intraoperative Complications
Intraoperative complications are an unavoidable risk of undertaking surgery. Whilst often unpredictable, a comprehensive preoperative assessment, good surgical insight, and adequate planning can lead to minimisation of risk and timely management of the pending complication to avoid future problems. This chapter reviews the common intraoperative complications encountered during simple extraction, and how they can be predicted and subsequently managed.
All forms of surgery require the use of traumatic instruments, in a controlled manner, in order to produce energy against the bodily tissues. This controlled tissue trauma minimises the damage done to the adjacent tissues during surgery, delivering a planned and predictable postoperative result. With the use of such instruments, however, comes the risk that trauma may instead occur in an uncontrolled manner. It is through this mechanism that most intraoperative complications occur.
Whilst safe practice and insight can minimise the risk of such complications, it is inevitable that the dentoalveolar surgeon will encounter each of those listed in this chapter at least once during their career. In such situations, the minimisation of harm to the patient is the goal of immediate management.
6.1 Lip Burns and Lacerations
The mobile lips and cheeks are the largest obstacle between the surgeon and the surgical site, and add an additional layer of difficulty compared with other forms of surgery. Lip lacerations usually occur as a result of inadvertent contact with the sharp metal instruments on their entry and exit from the oral surgical site. Lip burns are largely the result of inadequate retraction of the tissues when using a surgical handpiece. Both are significant complications, as they may cause long-term, visible external scarring or stricturing, in extreme cases requiring advanced facial plastic surgery.
If a lip burn or laceration occurs during a procedure, this needs to be evaluated immediately, before continuing with the planned surgery. The area should be examined for any obvious bleeding from the tissues and managed with firm pressure initially. All trauma must be clearly documented and described. Most importantly, the tissues involved – mucosa, vermillion, or skin – should be identified, as this will have a major impact on the prognosis of the patient.
Principles of Dentoalveolar Extractions, First Edition. Seth Delpachitra, Anton Sklavos and Ricky Kumar. © 2021 John Wiley & Sons Ltd. Published 2021 by John Wiley & Sons Ltd.
Companion website: www.wiley.com/go/delpachitradentoalveolarextractions
https://t.me/DentalBooksWorld